A safe environment for the client and other.
-
Workplace Safety
A safe environment for the client and other.
Workplace Safety.
Workplace safety refers to the working environment at a company and encompasses all factors that impact the safety, health, and well-being of employees. This can include environmental hazards, unsafe working conditions or processes, drug and alcohol abuse, and workplace violence. Workplace safety is monitored at the national level by the Occupational Safety and Health Administration (OSHA). OSHA has three stated goals that serve as the cornerstones of its policies and regulations: 1) Improve the safety and health for all workers, as evidenced by fewer hazards, reduced exposures, and fewer injuries, illnesses, and fatalities; 2) Change workplace culture to increase employer and worker awareness of, commitment to, and involvement in safety and health; 3) Secure public confidence through excellence in the development and delivery of OSHA’s programs and services. The federal guidelines imposed by this agency are complemented by state regulations that are often tougher than those proposed by OSHA.
Risk management refers to the practice of identifying potential risks in advance, analyzing them and taking precautionary steps to reduce/curb the risk.
Incident is an event or occurrence.
Accident is an unfortunate incident that happens unexpectedly and unintentionally, typically resulting in damage or injury.
Workplace hazards:
Physical hazards are the most common hazards and are present in most workplaces at some time. Examples include: frayed electrical cords, unguarded machinery, exposed moving parts, constant loud noise, vibrations, working from ladders, scaffolding or heights, spills, tripping hazards.Ergonomic hazards occur when the type of work you do, your body position and/or your working conditions put a strain on your body. They are difficult to identify because you don’t immediately recognize the harm they are doing to your health. Examples include: poor lighting, improperly adjusted workstations and chairs, frequent lifting, repetitive or awkward movements.
Chemical hazards are present when you are exposed to any chemical preparation (solid, liquid or gas) in the workplace. Examples include: cleaning products and solvents, vapours and fumes, carbon monoxide or other gases, gasoline or other flammable materials.
Biological hazards come from working with people, animals or infectious plant material. Examples include: blood or other bodily fluids, bacteria and viruses, insect bites, animal and bird droppings.
-
Environmental policies and procedures and their purposes.
A set of policies are principles, rules, and guidelines formulated or adopted by an organization to reach its long-term goals and typically published in a booklet or other form that is widely accessible.
Policies and procedures are designed to influence and determine all major decisions and actions, and all activities take place within the boundaries set by them. Procedures are the specific methods employed to express policies in action in day-to-day operations of the organization. Together, policies and procedures ensure that a point of view held by the governing body of an organization is translated into steps that result in an outcome compatible with that view.
Examples:
- Safety/risk management,
- Disaster plans,
- Bomb threat,
- Infection control procedures,
- Hazard communication,
- Radiation protection measures,
- Fire plan,
- Evacuation plan (floor/exit plan),
- Toxic chemical and MSDS (material safety data sheets) protocols,
- Oxygen usage.
Safety equipment is any equipment specifically designed to minimize injury or death. It might be built right into a product or it may be a stand-alone product.
Examples:
- Fire extinguishers.
- Eye wash station,
- PPE (personal protective equipment).
Environment safety hazards examples:
- Wet floors
- Cluttered paths of travel
- Unlocked wheels
- Side rails (Suffocation/asphyxia)
- Bed Elevation
- Improper shoes or dress
- Slippery surfaces
- Out-of-reach items
- Dim/reduced lighting
- Frayed cords
- Improper use of assistive devices
- Hot liquids/food
- Smoking
- Exposure to weather
- Uncontained chemicals
- Sharps
- Gas Leaks.
- Fire
-
Safety Management/Hazard Prevention.
Safety Management/Hazard Prevention
A direct care staff person provides care for clients in many ways. As you learned in the last module, knowing a client’s background helps you to assist the individual to be independent. A direct care staff person also needs to protect self and the client from accidents and hazards.
This session will help you to learn more about how to create a safe living environment. The two leading causes of unintentional injury and death for persons over the age of 65 years are fires and falls. However, there are other clients who, because of mental retardation, emotional or physical problems, are at risk for injury from accidents. Most of these accidents are caused by hazards in the environment and are preventable. An important aspect of prevention is to make sure that medications, chemical cleaners and any other poisons are kept locked.
The direct care staff person is responsible for knowing the regulations about fire safety and general safety. In this module you will learn to recognize common injuries, fire and fall hazards and steps you can take to keep the environment safe for yourself and clients.
SAFETY Here are some questions for you: How do you normally prevent accidents in your everyday life? How do you drink a cup of hot coffee without burning your mouth? How do you safely cross the street? The answer may seem so simple. The fact is you plan ahead. You try to think of what can go wrong and how you might keep things from going wrong. Before crossing a street, you stop, look both directions to see whether cars are coming, wait for any oncoming cars, and then you cross. Of course, even with good planning, things can go wrong. You will learn skills to help you prevent problems and know what to do in case an emergency does occur. It is impossible to cover everything, so only basic information will be presented about safety. You will need to learn what safety procedures are needed for your client. You might want to consider taking a first aid course from a local facility to further your knowledge and skills. Safety takes many forms: using equipment in such a way that you do not injure yourself or your care recipient; making the home safer from fire, from falls, or from poisoning; knowing when to call for help; or providing basic first aid care.
Preventive measures guiding principles:
- Gentleness, calmness;
- Slow and ‘steady as she goes;
- Eliminate/control of safety hazards;
- ACT (awareness, correction, take precautions);
- Inter-department communication
-
Common injuries.
Common injuries:
Sharp object injuries/skin tears
Explain dangers: occasionally workers may encounter needles, syringes, or razors on the job. Certain workplaces may be at a higher risk of encountering these types of hazards. The main risk to workers who have a needle stick injury is exposure to viruses such as hepatitis B and C, and human immunodeficiency virus (HIV).
- Hepatitis B is an illness that affects the liver. It causes liver inflammation, vomiting, and jaundice. Over the long term, it can cause scarring of the liver and liver cancer. It can eventually lead to death.
- Hepatitis C also affects the liver and can cause fever, loss of appetite, fatigue, and jaundice. Over longer periods of time, it causes scar tissue and liver failure. Some people may have no symptoms for many years but can still infect others.
- HIV is a virus that attacks the immune system, causing infection. When the body can’t fight infections anymore, the disease becomes acquired immunodeficiency syndrome (AIDS).
Identify controls: Use adequate lighting when working in dark areas to avoid any accidental contact with used needles or other sharp objects. Accidental contact with used needles can be avoided by following some simple procedures.
- If you find a needle or syringe, always assume it is contaminated.
- Before picking up the needle, notify your supervisor for direction. If your supervisor is not nearby, have another worker get the supervisor. Never leave the needle alone.
- Use a strong container (glass, metal, or durable plastic such as a peanut butter jar). Do not use pop bottles.
- Open the lid of the container and bring it close to the needle(s) or object(s). This will minimize the distance you have to carry the material.
- Use pliers, tongs, or tweezers to pick up the needle, syringe, or glass stem. Never use your hands.
- Hold the needle tip away from you at all times.
- Put the needle, syringe, or glass stem in the container.
- Close the lid securely.
- Do not dispose of needles in the garbage. Used needles should be dropped off at these designated locations. Your company may also have some other arrangement for disposal. Always follow your company’s disposal procedures.
Skin tears are traumatic injuries which can result in partial or full separation of the outer layers of the skin. These tears may occur due to shearing and friction forces or a blunt trauma, causing the epidermis to separate from the dermis (partial thickness wound) or both the epidermis and the dermis to separate from the underlying structures (full thickness wound). Skin tears are perceived by some to be minor injuries. However, they can be significant and complex wounds; complications such as infection or a compromised vascular status can increase morbidity or mortality risks.
What to do if you accidentally injured yourself?
- Let the wound bleed.
- Flush the area with water or wash with soap and water. If the skin has been broken, apply a topical antiseptic solution (e.g., iodine, isopropyl alcohol).
- Do not apply disinfectants to the eyes, nose, or mouth.
- Bandage the wound.
- Seek immediate medical attention at the hospital emergency department.
Muscle strains and sprains:
A sprain is a stretch and/or tear of a ligament, the fibrous band of connective tissue that joins the end of one bone with another. Ligaments stabilize and support the body’s joints. For example, ligaments in the knee connect the upper leg with the lower leg, enabling people to walk and run.
A strain is an injury of a muscle and/or tendon. Tendons are fibrous cords of tissue that attach muscles to bone.
A sprain is caused by direct or indirect trauma (a fall, a blow to the body, etc.) that knocks a joint out of position, and overstretches, and, in severe cases, ruptures the supporting ligaments. Typically, this injury occurs when an individual lands on an outstretched arm; slides into a base; jumps up and lands on the side of the foot; or runs on an uneven surface.
Chronic strains are the result of overuse (prolonged, repetitive movement) of muscles and tendons. Inadequate rest breaks during intensive training precipitates a strain. Acute strains are caused by a direct blow to the body, overstretching, or excessive muscle contraction.
Bruises:
A bruise also called a contusion (medical term), is a type of hematoma of tissue in which capillaries and sometimes venues are damaged by trauma, allowing blood to seep, hemorrhage, or extravagate into the surrounding interstitial tissues. Not blanching on pressure, bruises can involve capillaries at the level of skin, subcutaneous tissue, muscle, or bone.
Poisoning
Poison Prevention:
To prevent accidental poisoning consider the following:
- Store cleaning products properly;
- Never mix products together;
- If one product is put into another container, it should be relabeled;
- Make sure your care recipient is able to read the labels on containers;
- Lock up poisonous products for those who tend to be easily confused;
- Store all medications safely. They should be kept in their original containers, away from children, pets, and any heat sources;
- Cleaning tools and supplies should be stored safely as close as possible to where you will use them.
-
Fire
How do fires start?
For a fire to start, it needs four things:
- Fuel – Something that can burn.
- Heat – to ignite the material.
- Air – to keep the fire going.
- Chemical reaction – fire.
The first three are referred to as the “fire triangle.”
When you keep the first three separate, you prevent the chemical reaction (fire) from happening. For example, a lit cigarette (heat) falls into the trash (fuel) and the presence of oxygen in the air causes a chemical reaction (fire).
Fires are a serious threat to people who need assistance with moving quickly or have difficulty following directions. This is true of many clients of personal care agencies. Clients with mental illness or dementia, or who have functional impairments from any cause are at risk for injury. The risk increases dramatically with age. Persons 65 years of age and older are at two to five time greater risk to die in a fire than the rest of the population. What do you think causes these fires? Fires usually start from careless smoking, heating or cooking.
Careless smoking is the leading cause of fire deaths and second leading cause of injury for older persons. Fires from smoking frequently happen in early morning, afternoon or late evening when people are sleeping or relaxing. Just imagine––a person sits down to relax and lights a cigarette, becomes drowsy and falls asleep. The risk increases if a person drinks alcohol or takes medications that cause drowsiness. Fires can start when persons who are smoking are unattended or unsupervised. Sometimes the person forgets to put out the cigarette or doesn’t completely put it out and the cigarette continues to smolder. A client may never smoke in his/her bedroom. Smoking in rooms where oxygen is being used is also a hazard. Every home is required to have smoking safety procedures and policies.
Cooking is the leading cause of injury from fire and the third leading cause of death. Here are some specific cooking-related dangers:
- A person leaves a hot stove unattended for just a few seconds to answer the phone or to help someone in another room.
- Persons wear loose fitting clothing or long flowing sleeves while cooking.
- A person leaves hot mitts or paper towels near a hot stove and they ignite.
- The person cooking forgets to turn off appliances.
- The person leaves pot handles extending over the front of the stove where they can bump into them, causing a serious scalding burn. Turn all pot handles to the side or back of stovetop.
Heating is the second leading cause of fire death and third leading cause of injury. Most of these fires occur in months when the weather is cold and heating devices such as space heaters, fireplaces and wood stoves are used to add extra warmth. Portable space heaters are very dangerous and cause fires. Secure screens and protective guards are required for fireplaces and wood and coal burning stoves. If your client home has any of these heating sources, you will want to keep flammable items, such as newspapers or cleaning fluids, away from the heating source.
Another source of fires is faulty electrical equipment. Electrical appliances are often used in cooking. You may also be using electrical appliances in the process of assisting clients with their activities of daily living. Some safety measures you can take to prevent electrical fires are:
- Check all electrical appliances for frayed cords or damaged plugs before using.
- Avoid overloading electrical circuits by plugging in numerous cords.
- Do not try to repair electrical equipment yourself.
- If an electrical appliance begins to “smoke,” turn it off, unplug and remove it.
- Unplug a countertop appliance when the appliance is not in use.
Since oxygen is one of the three things needed for fire to start, the presence of extra oxygen in the home when persons use oxygen is a special concern. You will want to make sure there is no smoking in areas where oxygen is being used. Matches, lighters, smoking materials and other flammable products like nail polish, alcohol and oils should be removed. Wool and synthetic clothing can create static. Clothing made of cotton is best to eliminate the risk of static and sparking. Electrical equipment like radios, toys and razors, can also create sparks.
-
What should the direct care staff person do if there is a fire
If there is a fire in the building where you are now going through this training program, what would you do? The right course of action is for you to act quickly and R.A.C.E. to respond to the fire.
The R.A.C.E. response for the direct care staff person is to:
- Remove any clients or other persons near the fire.
- Activate the alarm to notify others that there is a fire.
- Confine the fire by closing doors as you exit the room.
- Exit. All clients in the home must quickly evacuate outside the building (or in some homes, to a fire safe area inside the home).
All personal homes are required to have operable smoke detectors or fire alarms to alert you of fires. Some homes may have sprinkler systems. Knowing where this equipment is located is necessary in the event you need to activate an alarm. Look for detectors in the hallways and outside the bedroom doors. You will also want to learn if there are any clients with hearing impairments who are dependent on signaling devices like vibrating beds or strobe lights to warn them of emergencies.
How do you use a fire extinguisher?It is important for you to learn the location of the extinguishers, and how to unlock and use them. Newer fire extinguishers use the picture/labeling system to designate which types of fires they are to be used on. Older fire extinguishers used the label with colored geometrical shapes with letter designations.
Think of the word PASS to learn to use a fire extinguisher:
P – Pull the metal pin on the upper handle.
A – Aim at the base, or the bottom, of the fire or flame.
S – Squeeze the handle while holding the extinguisher up straight.
S – Sweep from side to side while still aiming at the base.
A direct care staff person should not use a fire extinguisher to fight a fire. It should be used only to clear an exit path or put out a fire on a person.
How do you plan for a fire emergency?The best way is to prepare yourself and the clients for an emergency before it happens. How do I assess the care recipients’ home for fire safety? Some of the things you should be aware of when assessing a home for fire safety include:
- Are there smoke detectors and are they working? The batteries should be checked periodically.
- Install a fire extinguisher if there isn’t. Check them periodically according to the manufacturer’s directions.
- Check electrical cords for fraying or for broken prongs. Also, be sure there aren’t too many cords plugged in to one outlet. Some appliances should be unplugged when they are not in use.
- Have an emergency plan for how to exit the home in an emergency. Decide on a meeting place outside in case a fire does occur. Also, plan an alternate exit route.
- Use common sense when cooking. Never leave cooking unattended on the stove. Don’t wear loose-fitting sleeves when working around the stove. Turn off the burners and oven when you are done using them. Turn handles toward the back of the stove when cooking.
- Encourage appropriate smoking habits. Never smoke in bed. Smoking should NEVER be allowed around oxygen. Make sure the care recipient uses acceptable ashtrays, preferably with notches on the side to hold cigarettes. Ensure ashtray contents are disposed of properly.
- Remembers the STOP, DROP, and ROLL rule. (If clothing catches on fire, stop immediately, drop to the ground, and roll to smother flames).
- Check the home for hazards such as: excess papers or rags; improperly stored cleaning products, paint, and chemicals; faulty space heaters or heating pads.
Whenever you observe any safety hazard, follow the agency policy for reporting it. Every personal home apartment has a fire evacuation plan. Here are some other things you will need to know to help yourself and the residents move quickly to safety:
- How to contact local fire and emergency services.
- The location of the exits – there are at least two independent and accessible exits on every floor.
- The location of the escape routes and how to evacuate the home. These routes must be unlocked and clear at all times.
- How to assist clients with mobility needs during an evacuation.
-
Falls
Slip, trip and fall prevention:
Can you remember a time when you had a bad fall or tripped over something in your path? It happens so fast! Were you able to recover quickly or did it take a while? Falls are the leading cause of injury and death for older people. They are the most common cause of non-fatal injuries and hospital admission for trauma. When an older person falls, his/her ability to function physically can be decreased and he/she may become permanently disabled. This loss of independence can lead to further decline in physical abilities, depression, feelings of helplessness and social isolation.
What are the common causes of slips, trips and falls?
Think about a time when either you or someone you know slipped, tripped or fell. How did it happen? Take a look around the room you are in now. Do you see any hazards that could result in someone tripping, slipping or falling?
Some of the common causes of falls include the following:
- Frayed carpet and slippery rugs.
- Loose tiles or lifted edges of floors.
- Wet floors.
- Cluttered hallways or paths.
- Shoes, slippers or socks that are slippery.
- Ice or snow.
- Poor lighting, including burnt-out light bulbs.
- Loose or missing handrails on staircases.
- Slipping in bathtubs or showers.
- Trying to get out of bed or a chair without necessary assistance.
Other hazards are unlocked safety brakes on wheelchairs and broken walkers or canes. These are all devices that may be used by older persons to assist them in remaining as independent as possible. The risk of falls increases when older persons take medications that cause drowsiness or dizziness or have physical weakness and walking problems.
What can the direct care staff person do to reduce the risk of slips, trips and falls?
If you think about the causes of slips, trips and falls, you will think of answers to reducing them. For example, if throw rugs cause tripping, remove them and replace them with safer carpeting or non-slip flooring. Let’s look at some additional ways to reduce slips, trips and falls:
- Use wheelchairs to provide safe mobility.
- Encourage clients to use grab bars, raised toilet seats, adjustable bed heights and handrails in hallways to help them get up and down and move from one place to another safely.
- Make sure all cords, including extension cords do not lay where people walk.
- Remove hall clutter.
- Check to see that stairways are well lit so that each step, particularly the step edges, can be clearly seen by the clients while going up and down the stairs. The lighting should not produce glare or shadows along the stairway.
- Use the maximum wattage bulb allowed by the light fixture. If you are uncertain about the recommended wattage, use a 60-watt bulb or lower.
- Do not store anything on the stairs, even temporarily.
- Ensure that handrails are sturdy and fastened securely on both sides of the stairway.
- Help clients remain mobile by encouraging them to do exercises that build up leg muscle (walking, tai chi, etc.). This is one of the best ways to prevent falls.
- Use rubber mats and slip-proof tub mats inside and outside bathtubs and showers.
- Be attentive to the client’s need for assistance to get into or out of bed and in and out of a chair.
- Keep a night light on in the client’s room so they can get to the bathroom safely. (Nighttime rising to go to the bathroom is a common time for falls.)
- Wipe up spills immediately – liquids, snow, mud, sugar, salt, powder.
- Keep frequently used items easily available – telephone, remote controls, tissues, etc.
- Clear walkways of obstacles.
- Install grab bars in bathrooms and hallways. Encourage the care recipient to use them.
- Remind the care recipient to wear proper footwear with rubber soles.
- Lock the wheels on wheelchairs when transferring.
- Encourage exercise to maintain strength.
- If the care recipient has pets, watch for them when walking.
- Make sure the furniture is the right height. Armrests are helpful for getting in and out of chairs.
- Check stairways for clutter, handrail stability, step width, and safety.
- Don’t move any of the furniture. .
- Remind the care recipient to allow enough time to get to the bathroom for toileting so he/she doesn’t have to hurry.
- Remember safety outside of the home. Check lighting, steps, handrail stability, and for items the care recipient could trip on.
Falls can cause moderate to severe injuries, such as hip fractures and head traumas, and can increase the risk of early death. Fortunately, falls are a public health problem that is largely preventable. Whenever you observe any safety hazard, follow the agency policy for reporting it.
-
Falls facts
Each year, millions of adults aged 65 and older fall:
- One out of three older adults (those aged 65 or older) falls each year, but less than half talk to their healthcare providers about it
- Among older adults, falls are the leading cause of both fatal and nonfatal injuries.
- In 2013, 2.5 million nonfatal falls among older adults were treated in emergency departments and more than 734,000 of these patients were hospitalized.
- In 2013, the direct medical costs of falls, adjusted for inflation, were $34 billion.
- Twenty to thirty percent of people who fall suffer moderate to severe injuries such as lacerations, hip fractures, and head traumas. These injuries can make it hard to get around or live independently, and increase the risk of early death.
- Falls are the most common cause of traumatic brain injuries (TBI).
- About one-half of fatal falls among older adults are due to TBI.
- Most fractures among older adults are caused by falls.
- The most common are fractures of the spine, hip, forearm, leg, ankle, pelvis, upper arm, and hand.
- Many people who fall, even if they are not injured, develop a fear of falling. This fear may cause them to limit their activities, which leads to reduced mobility and loss of physical fitness, and in turn increases their actual risk of falling.
Fall-related Deaths
- The death rates from falls among older men and women have risen sharply over the past decade.
- In 2013, about 25,500 older adults died from unintentional fall injuries.
- Men are more likely than women to die from a fall. After taking age into account, the fall death rate is approximately 40% higher for men than for women.
- Older whites are 2.7 times more likely to die from falls as their black counterparts.
Assisting the falling client:
Care of the client after falling:
Transfer of the patient to a hospital emergency room is appropriate if he or she exhibits the following injuries or signs after a fall:
- Uncontrolled bleeding
- Major fracture or fracture likely to require surgical intervention
- Deformity of limbs
- Acute change in neurological status or cognition.
-
Client related safety measures
Common causes of accident in the older population:
- Age;
- Medication;
- Poor mobility;
- Sensory impairment;
- Confusion or limited awareness of surrounding.
Client related safety measures:
Assessments and identifying needs.
Assessment Process: What will help the client remain in the home?
1. Referralinformation:
ü Diagnosis, medical history.
ü Other;
2. Homevisit;
ü Patient/family interview: self-identified, statedneeds.
3. Psycho-social,environmental, physicalassessment.
4. Intuitive nature of assessment from experiencedassessors.
Living Arrangements
- Own home, apartment, assisted living
- Condition of home (clean/dirty, cluttered, safety hazards, Structural barriers,
- Bathing facilities tub, shower
- Lives with someone? Who?
- Responsible person?
- Type and Frequency of assistance needed
- Resources finances
Client’s Level of Functioning
- Functional Limitations, activities allowed, assistance needed
- Mental status and functioning: oriented, forgetful, depressed, agitated, memory, decision- making,
- Motivation
- Ability to bathe, dressing
- Toileting
- Ambulation, transferring ,
- Feeding/eating
- Transportation, shopping, money management
- Medication and equipment management
Common Needs of Home Care Clients
- Nutritional needs
- Dementia, behavioral
- Functional/mobility impairments
1. Loss of function;
2. Size of patient.
- Communication impairments
1. Speech, hearing, language.
- Companionship
1. Referralinformation:
ü Diagnosis, medical history.
ü Other;
2. Homevisit;
ü Patient/family interview: self-identified, statedneeds.
3. Psycho-social,environmental, physicalassessment.
4. Intuitive nature of assessment from experiencedassessors.
-
Some common problems that are associated with clients…
Some common problems that are associated with clients, and offers some suggestions for providing effective care.
Agitation Restlessness Anxiety.
- Speak in a calm voice, remove noise and distractions. Avoid abrupt movements.
- Establish a routine and stick with it.
- Offer repetitive, familiar tasks, like folding towels, sorting things, looking at pictures.
- Play soft music.
Lack of understanding of language.
- Repeat yourself.
- Use simple phrases and messages.
- Break down complex tasks into small, simple ones.
- Use pictures and gestures
Lack of judgment regarding safety.
- Be aware of safety concerns in the home, report them to the supervisor.
- Use gates, close doors and windows, remove clutter.
- Keep areas well lit. Post signs or pictures (STOP signs on outside doors, picture of the toilet on bathroom door).
- Put stickers or colored tape on clear glass doors and windows to avoid walking into the glass.
- Use locks on doors or alarms that will sound when the door is opened.
- Be sure the client wears some form of identification: a bracelet, ID label, etc.
- Keep chemicals and medications out of sight and out of reach.
- Remove knobs on the stove, unplug small appliances.
- Check the refrigerator for spoiled food.
- Use non-skid mats in the bathroom.
- Do not leave client unattended.
Lack of awareness for self-care needs
- Encourage client to care for self asmuch as possible, offering reminders and simple directions.
- Don’t give too many choices about when to bathe, what to wear.
- Be directive.
Memory loss Disorientation to person, place, or time.
- Use calendars.
- Write notes.
- Keep pictures & familiar objects in view.
- Do not move furniture around.
Hallucinations
- Ignore them, if harmless.
- Reassure the client who is worried.
- Do not argue about the reality of what he sees or hears.
- Try to re-direct activity. Remain calm.
Catastrophic Reaction/Event
- Try to determine what caused the unreasonable reaction: fatigue, change in routine, noise, too much stimulation, pain, hunger, and need to toilet.
- Try to remove triggers.
- Remain calm and reassuring.
- Call for help as necessary.
- Provide for your own safety.
Resistance to bathing
- Try to preserve familiar routines. If the person always showered in the morning, continue to offer that rather than a tub bath in the evening.
- Give simple directions, not choices: “Take off your shirt. Now take off your pants. Now step into the shower.”
- Never leave the client alone.
Refusal to eat
- Check for dental pain or other illness.
- Offer one food at a time.
- Cut into small pieces.
- Serve food attractively, in good lighting.
- Play soft music.
- Offer food again in a few minutes.
Frustration, Depression
- Report signs of depression to supervisor: aches and pains, low energy, sleeplessness or excessive sleeping, lack of interest.
- Encourage self-care and independence.
- Encourage social interaction
- Listen.
Violent behavior
- Block his blows.
- Do not hit back. Step out of reach.
- Do not leave client alone.
- Call for help as necessary.
- Offer reassurance, using calm voice.
Repetitive phrases, like, “I want to go home.”
- Be patient.
- Allow client to repeat himself.
- Respond each time with same phrase.
- Attempt to distract with new activity.
- Do not argue with him or try to silence him.
Incontinence
- Assist to toilet every hour or two.
- Maintain regular schedule for toileting.
- Record bowel movements.
- Check skin for redness or breakdown.
- Assist with peri care as necessary.
- Keep skin clean and dry.
Wandering Pacing
- Try to determine whether he is uncomfortable due to hunger, need for toileting, need for exercise.
- Remove the cause if possible.
- Provide safe path.
Inappropriate sexual behavior.
- Ignore remarks.
- Offer distractions, other activities change the subject.
- Offer privacy.
- Realize that this is part of the disease.
- Exposing oneself could signify:
1. need to toilet;
2. forgot to get dressed;
3. is too warm.
Hiding and hoarding things.
- Don’t leave things lying around.
- Look through wastebaskets before emptying them.
- Look frequently in his usual hiding places.
- Keep the home uncluttered.
Lack of recognition for own health needs
- Observe and report changes & areas of concern to supervisor.
- Offer familiar foods and frequent liquids.
- Monitor weight.
-
Support Plans
Introduction:
It is important to work as a TEAM. As a direct care staff person, you are one of the primary caregivers for the clients in their home. However, you are not alone. You are part of a care TEAM that must work together to provide the best possible care. The members of the care TEAM will vary depending on the size and organizational structure of the personal care home. At a very small personal home care agencies, there may be only an administrator, a few direct care staff persons and the clients. Large personal home care agencies may have directors, supervisors, specialists, personal care workers and nutrition staff.
At the center of the care TEAM is the client and his/her needs and preferences. A TEAM, when it works together well, can provide better and more comprehensive care to a client than staff members working separately. Think of a TEAM, any kind of TEAM. It could be a group to which you belong, a sports TEAM on which your child plays or one you see on TV. What makes that TEAM work well? Maybe they win, have good sportsmanship, do something to help others or simply complete what they set out to accomplish. Effective TEAMS have the following traits:
- Work toward a common goal.
- Talk to each other.
- Support one another.
- Share responsibility.
- Strive to improve.
Common goal:
Working on a TEAM means having a common goal that is shared by everyone. What is the goal of the personal home care TEAM?
Communication (or talking) is the glue that keeps the TEAM on track toward its goal. Your communication with the client is important to learning about the kind of life he/she wants and how you can best assist the client to achieve that lifestyle. To your supervisor, you communicate changes you see or learn from the client. With co-workers you share ideas on better ways to do a task, or get/lend a helping hand. Knowing that you’re not alone can make your job much more satisfying.
Your role on the care TEAM:
As a direct care staff person, you play a key role on the care TEAM because you provide the day-to-day care for clients. You may see more than anyone else about what is going on with an individual. You are responsible for contacting your supervisor or others on the care TEAM as directed to get the help any client needs. You will provide important information to the rest of the care TEAM through your daily observations, reporting and documentation. You can help maintain your awareness of a client’s care needs by following these steps:
- Watch for changes. Notice changes that may signal the need for special attention or additional care.
- Regularly review with your supervisor, and with staff on the previous shift, any written documentation (such as client’s charts, progress notes and medication record) for updates on a client’s needs.
- Report and document all changes. Report changes in a client’s needs.
Initial and annual assessment:
An initial assessment is done with each new client .This assessment gives a snapshot of the client’s preferences and needs for assistance. The client, family members, physicians and current caregivers are all asked to share information as part of the assessment so that the home can develop a good support plan.
The client is asked about his/her need for assistance with ADLs and IADLs, communication, medication administration and mobility. The client’s mental health and memory are assessed. The need for health and social services are noted. The client’s choices, preferences for activities, religious practice, like and dislikes are listed. This assessment is done each year or more often if the needs of a client change.
Support plans:
Each personal home care agency has support plans that show the special needs and services for each client including medical, dental, vision, hearing and mental health services. It explains the client’s ability to take their medications and how staff should assist. The plan will explain if the client needs help to walk, bathe or dress and the type of help he/she needs. The plan will also explain the social activities and other services that are specially designed for each client. The support plan must be accessible by direct care staff persons at all times.
-
1. Responds to Medical emergency situations:
Injury Prevention
Emergency Situations and Critical Incidents
Medical Emergency, Major Trauma, or Life Threatening Incidents:
Occasionally, an employee may encounter an unusual, unexpected, or emergency situation in the home. The employee is required to act according to the nature and severity of the incident.
- Call 911 immediately.
- Report what has happened to the office.
- The Administrator/Manager will notify the client’s emergency contact and the physician.
- Stay with the client until help arrives and the situation is under control.
Non-Life Threatening Incidents:
- Make the client comfortable.
- Inform the office and the family.
- Follow the Administrator/Manager’s instructions.
Incident Reports:
Immediately following an incident, the employee involved must complete an incident report form and review the incident with the supervisor. Examples of incidents which must be reported include but are not limited to client complaints, accidents and/or injury to employees or clients, equipment or medical device failure or malfunction, theft, suspicion of abuse, neglect or exploitation, and criminal activity.
- The supervisor will follow up on any reported incidents as appropriate.
- Actions taken and resolutions of identified problems will be documented.
- A log will be kept of all incidents.
- Incident reports and logs will be reviewed on an ongoing basis to note trends.
INJURY PREVENTION
In order to reduce accidents and injury to staff, environmental conditions should be monitored, potential hazards and risks should be identified, and staff should be educated in maintaining a hazard-free environment, as follows:
Office Safety
- Employees are responsible for keeping their work areas neat and orderly.
- Equipment, supplies, and furniture are used, stored, and maintained in a safe manner.
- Regular safety survey reviews and correct housekeeping practices as applicable.
- Staff is instructed to report any known or suspected hazards to their supervisors.
- Safety practices are reviewed regularly for potential hazards in the office environment.
Hazard Assessment and Control
Fire Prevention
- Local, county, and district Fire Departments are consulted for codes and ordinances.
- Fire drills are held periodically.
- Staff is instructed to meet at a specific safe location outside agency premises in order to count employees and determine that everyone has safely evacuated the building.
- Fire extinguishers are inspected and maintained regularly.
- Fire evacuation routes are posted conspicuously in prominent locations.
- Employees are educated in fire prevention, evacuation, and use of fire extinguishers.
Pertinent Safety Issues
- Employees are educated regarding their roles in emergency and disaster situations.
- During joint home visits, home safety practices are evaluated as part of performance evaluations.
- Motor vehicle safety and proper use of cell phones are stressed.
- Employees are schooled in Ergonomics and body mechanics related to job performance.
- Employees are educated in electrical safety as it relates to medical equipment.
- Safety issues are presented at orientation, in-services, and at regular meeting.
- Memos, flyers, and bulletin boards are used to communicate safety issues.
- Safety materials and practices are reviewed and modified annually
Safety Communications
- Safety issues are presented at orientation, in-services, and at regular meeting.
- Memos, flyers, and bulletin boards are used to communicate safety issues.
- Safety materials and practices are reviewed and modified annually
-
2. Responds to Medical emergency situations:
How do I handle emergency situations?
In an emergency situation, it is sometimes hard to know when to call for help. A general rule of thumb is to call the fire department, ambulance, or police if you have to ask yourself whether or not you should call. Your instincts will usually let you know when you need help. Know the emergency numbers in your care recipient’s area. Most areas use the 911 system. If they do not, write down the numbers ahead of time and have them posted by the phone. The numbers you should have readily available may include: doctor, poison center, fire department, police, and family and friends. First Aid In general, you should NEVER move the care recipient when an accident has happened. Moving them may result in further injury. Of course, if there is immediate danger to the care recipient, such as a fire, then you should.
Signs of Medical emergencies:
- Airway obstruction (choking);
- Heart attack;
- Brain attack;
- Fainting;
- Seizures;
- External hemorrhage;
- Shock.
Responds to Medical emergency situations.
- Heimlich maneuver, CPR (CPR and the Heimlich maneuver are not covered in this course. It is recommended that you get this training from qualified personnel. Most hospitals and ambulance services offer the training periodically. Check in your area for classes).
- Call 911.
- Positioning when fainting.
- Fainting is a medical emergency, till proven otherwise
- When a person feels faint-
- Make them sit down or lie down
- If sitting, position head between knees
- When a person faints, position him on his back
- Check to see if airways are clear
- Restore blood flow by
- Loosening clothing/belts/collars
- Elevate feet above head level
- Patient should become normal within a minute
- If not, seek medical help
- Check if breathing/pulse is normal
- If not, do CPR
Providing safety during seizures.
Protect a head. The recovery position may be necessary to prevent chocking (aspiration vomitus) or to promote breathing (preventing a collapsed airway):
- Kneel beside the victim and place both of the person arms close to his or her body.
- Turn the person gently onto the side.
- Draw the upper arm and leg upwards and outwards to form right angles with the body. This prevent the person from rolling forward.
- Pull the underneath arm out gently behind the person. This prevent the person rolling backward.
Applying pressure when bleeding.
The most common first aid procedure you may have to perform is caring for bleeding.
The basic principles are:
- Cover with a clean cloth
- Apply pressure
- Elevate the area
- Do NOT remove any object stuck in the site, such as glass.
- Do NOT remove original bandage, cover with another one if needed.
Recognize shock Recognize shock, heart attack, and stroke.
The shock signs include:
- Pale, cold, and clammy skin
- Person may feel sick or actually vomit
- Person may complain of feeling thirsty
- Pulse speeds up but is weaker
- Respirations become faster and more shallow
You will need to treat shock right away if these signs develop. After calling for an ambulance, treatment includes doing the following:
- Lay the person flat, with the legs elevated, if possible
- Cover the person with a blanket to keep warm
- Do NOT give the person anything to drink, but you can moisten the lips slightly
- Loosen clothing for better breathing and comfort.
The heart attack, and stroke signs:
- Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain.
- Shortness of breath.
- Cold sweat, nausea or lightheadedness.
- Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach.
Face Drooping Does one side of the face droop or is it numb? Ask the person to smile
Arm Weakness Is one arm weak or numb? Ask the person to raise both arms. Does one arm drift downward?
Speech Difficulty Is speech slurred, are they unable to speak, or are they hard to understand? Ask the person to repeat a simple sentence, like “the sky is blue.” Is the sentence repeated correctly?
Time to call 9-1-1 if the person shows any of these symptoms, even if the symptoms go away, call 9-1-1 and get them to the hospital immediately.
In Case of emergency stay calm and take immediate action to remove clients from danger!
-
Body Mechanics
Transferring, lifting, moving, and positioning care recipients can be a major safety problem unless you learn how to use good body mechanics. ‘Body mechanics’ involves how you stand, move, and position your body to prevent injury, avoid fatigue, and make the best use of your strength. Understanding the principles of good body mechanics and applying them to your everyday routine, whether at home or at work, enables you to feel better and less tired at the end of the day.
What are the principles of body mechanics?
Body mechanics involves using good posture, balance, and the strongest and largest muscles of the body to perform the work. You can lift and move easier, no matter what your size is. You need to be concerned with both your own body mechanics and that of the care recipient. The major movable parts of the body are the head, trunk, arms, and legs. The way in which they are aligned with each other is known as posture or body alignment. Proper body alignment allows us to move and function efficiently and with strength whether we are standing, sitting, or lying down. Base of support is the area upon which an object rests. In humans, this is the feet. We need a good base of support in order to maintain balance. Standing with one’s feet apart gives a wider base of support and, therefore, more balance and stability. The strongest and largest muscle groups of the body are located in the shoulders, upper arms, hips, and thighs (NOT in the back.) By using smaller and weaker muscles to move heavy objects, you strain them, causing fatigue and injury. Use the strong muscles of your thighs and hips by bending your knees and squatting to lift a heavy object. Avoid bending from the waist when lifting, as this involves the small muscles of the back. Holding objects close to the body and base of support involves using upper arm and shoulder muscles. Holding an object away from the body exerts strain on the smaller muscles of the lower arms.
Follow these guidelines when lifting, moving, and transferring care recipients:
- Stand close to the care recipient.
- Create a base of support by placing your feet wide apart.
- Make sure the area is safe for a move or a lift.
- Bend at your hips and knees with your back straight.
- Push up with your leg muscles to a standing position. Back injuries are not usually the result of one incident but of the constant use of smaller back muscles.
DON’T Lift With Your Back, Lift With Your Head!!!!!!
TRANSFERS AND ASSISTIVE DEVICES
Lifting and Back Protection
Every effort is made to protect employees from injury, but they must also use good judgment to avoid injuries. The most common injury to health care workers is a back injury. Employees are encouraged to strengthen their backs through daily exercise in order to prevent injuries.
Employees are prohibited from moving heavy objects in clients’ homes that may result in injury. For example, employees must not move refrigerators, televisions, heavy furniture, heavy boxes, etc. If a client requests this, the employee should refuse and report the request to the Supervisor.
If a client or employee is injured during a home visit, or if there is evidence of a safety or fire hazard, the employee must report the situation to a supervisor immediately.
Back Protection and Good Body Mechanics Guidelines
“Body Mechanics” is using the body in an efficient and careful way to save energy and prevent injury. It includes good posture, balance, and using the strongest and largest muscles to do the work. “Body Mechanics” is the way a body moves and keeps its balance through the use of all its parts.
“Posture” is another word for “body alignment”. Good posture means keeping major body parts, including head, trunk, arms, and legs in a straight line to allow the body to move and function with strength and efficiency.
“Base of support” is the foundation for an object or individual. A human being’s feet are the person’s base, their source of support and balance. When the feet are wide apart, the person’s “base of support” is at its most stable foundation.
Our strongest and largest muscles are in the shoulders, upper arms, hips, and thighs. These muscles should be used to lift and move heavy objects and clients. If small and weaker muscles (lower back, neck, lower arms) are used for lifting, they could be injured. Objects being held or carried should be kept close to the navel (“center of gravity”) where the strong muscles will best support them. Holding them away or at an angle places unnecessary strain on the lower arms and back, causing fatigue and injury.
Basic Rules for Back Protection
- Plan ahead. Know what you will be moving and where.
- Know your limits. Evaluate the risks to you and the client.
- Keep your back steady and body parts in good alignment.
- Keep your feet apart to provide a broad base of support.
- Bend from the knees, NOT from the waist.
- Squat to lift objects from the floor.
- Lift with your legs, NOT with your back.
- Pivot your whole body to turn. Do not twist or reach.
- Keep objects and clients close to your body when moving or lifting them.
- Use the strongest muscles to do the job; shoulders, hips, legs, and upper arms.
- Instead of lifting, push, slide, or pull heavy objects whenever possible.
- Synchronize movements with client. Count “l , 2, 3″and work together.
- Work with smooth and even movements. Avoid sudden or jerky motions.
- Practice until you feel confident.
Helping a Reclining Client Sit on the Side of the Bed
- Explain the procedure and ask the client to do as much as possible for themselves.
- Wash your hands. Provide for privacy. Gather robe and non-skid shoes.
- Determine which side of the bed to use. Always move toward the client’s strong side.
- Ask the client to move toward the side of the bed. Assist as necessary.
- Keep your knees flexed and back steady. It may help to put one knee on the bed toward the client’s head. Slide one arm under the client’s neck and shoulders.
- Grasp the far shoulder. Place your other hand under the client’s far knee.
- Guide the client’s legs over the edge of the bed while supporting the shoulders toward an upright position. Move the client in a fluid, smooth manner. .
- Ask the client to put their hands or fists on the mattress to support themselves in a sitting position.
- Be sure the client’s feet are flat on the floor and you are preventing their feet from sliding.
- Provide continued support as necessary.
- Allow time for the client to become balanced and steady in the sitting position.
- Do not move away until the client is sitting independently.
- Do not leave the client i f there is any chance they will fall forward or backward.
Stand-By Assistance (“Contact-Guard”)
Some clients with weakness, mobility, or balance problems will need a help to accomplish the activities of daily living. The Personal Care Provider will assist these clients by “standing by” or “guarding with contact” as they change positions, while the client steps into the shower, or walks about the home. A stand-by assist is accomplished with the PCP/PCW at the client’s weaker side or back, with a guiding hand on the person’s elbow, around the waist, or with fingers in the belt loops, or under the transfer belt. Sometimes a verbal reminder is useful to cue the client regarding which foot to move, which direction to move toward, or where to hold on for support. The PCP/PCW, who pays close attention to the client’s movements and is ready to lend a hand whenever necessary, provides “stand-by” assist.
-
Taking care of the client receiving Oxygen
Oxygen sources:
1. Wall outlet
2. Oxygen tank

3. Concentrator

4. Oxygen cannula/prongs
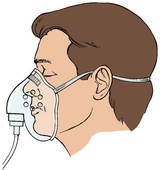
5. Oxygen mask
Oxygen Therapy Safety Precautions
- Place cautionary signs reading “No Smoking: Oxygen in Use” on the client’s door, at the foot or head of the bed, and on the oxygen equipment.
- Handle and store oxygen cylinders with caution, and strap them securely in wheeled transport devices or stands to prevent possible falls and outlet breakages. Place them away from traffic areas and heaters.
- Instruct the client and visitors about the hazard of smoking with oxygen in use. Teach family members and roommates to smoke only outside or in provided smoking rooms away from the client.
- Make sure that electric devices (e.g., razors, hearing aids, radios, televisions, and heating pads) are in good working order to prevent the occurrence of short-circuit sparks.
- Avoid materials that generate static electricity, such as woolen blankets and synthetic fabrics. Advise clients and caregivers to wear cotton fabrics and use cotton blanket.
- Avoid the use of volatile, flammable materials, such as oils, greases, alcohol, ether, and acetone (e.g., nail polish remover), near clients receiving oxygen.
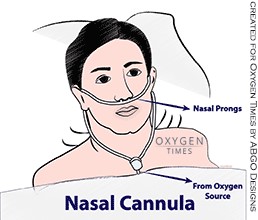
Assisting with nasal cannula.
- Hold nasal cannula in proper position with prongs curving downward.

Fig. 7: Properly position nasal cannula with prongs curving downward.
- Place cannula prongs into nares.

Fig. 8: Place cannula prongs into nares.
- Wrap tubing over and behind ears .

Fig. 9: Wrap tubing around ears.
- Adjust plastic slide under chin until cannula fits snugly.

Fig. 10: Adjust plastic slide under chin until cannula fits snugly.
- Place gauze at ear beneath tubing as necessary (Fig. 11).

Rationale: Proper placement in nares ensures accurate administration. Note: The cannula permits some freedom of movement and does not interfere with the client’s ability to eat or talk.
Fig. 11: Place gauze at ear to reduce irritation and promote comfort.
- If prongs dislodge from nares, replace promptly.
Rationale: To ensure correct oxygen delivery and prevent hypoxemia.
- Assess for proper functioning of equipment and observe client’s initial response to therapy.
ASSISTING WITH THE USE OF THE OXYGEN CONCENTRATOR
- Explain procedure to client.
- Wash hands.
- Assemble equipment.
- Clean air filter.
- Wash humidifying bottle, if used.
- Check the humidifying bottle to make sure it has an adequate amount of distilled water in it, and the bottle is screwed on tightly, if used.
- Attach the air tube, if not on, to the humidifying bottle or oxygen concentrator.
- Take and records the client’s pulse and respiratory rate.
- Turn on the switch to the oxygen concentrator.
- Check that air is bubbling through the humidifying bottle.
- Check that air is flowing through the nasal cannula.
- Ensure that flow meter is set to appropriate level as noted in the care plan. (REGULATION OF FLOW METER DONE BY AIDE UNDER SPECIAL CIRCUMSTANCES ONLY.)
- Assist the client in applying the nasal cannula.
- Take and records the client’s pulse and respiratory rate.
- Turn off the oxygen concentrator.
- Assist the client in removing the nasal cannula.
- Wash hands.
- Observe for difficulty breathing; rapid pulse and respirations; cold, clammy skin; blue or darkened lips, fingernails, eyelids; client unable to sit still; client does not respond when you call client’s name, has headaches; or complains of no energy.
ASSISTING WITH THE USE OF THE OXYGEN TANK AND LIQUID OXYGEN RESERVOIR
- Explain procedure to the client.
- Wash hands.
- Assemble equipment.
- Put on gloves, as necessary.
- Check oxygen tank or reservoir gauge to see if there is enough oxygen. Call supplier if not.
- Wash humidifying bottle.
- Check the humidifying bottle to make sure it has an adequate amount of distilled water in it, and the bottle is screwed on tightly.
- Take and record the client’s pulse and respiratory rate.
- Turn on the oxygen tank.
- Ensure that flow meter is set to appropriate level as noted in the care plan. (REGULATION OF FLOW METER DONE BY AIDE UNDER SPECIAL CIRCUMSTANCES ONLY.)
- Check that water in humidifying bottle is bubbling.
- Check that air is flowing from the mask or nasal cannula.
- Assist the client in applying mask or nasal cannula.
- Cannula: prongs go into nose.
- Mask: should fit close to face, but not pinch it.
- Take and record the client’s pulse and respiratory rate.
- Turn oxygen tank off
- Turn the flow meter off.
- Assist the client in removing the oxygen mask or nasal cannula.
- Wash hands.
- Observe for difficulty breathing; rapid pulse and respirations; cold, clammy skin; blue or darkened lips, fingernails, eyelids; client unable to sit still, client does not respond when you call his/her name; has headaches; or complains of no energy.
- Record the use of the oxygen tank or liquid oxygen reservoir and observations of the client.
- Report to supervisor IMMEDIATELY if client has difficulty breathing; has rapid pulse and respirations; has cold, clammy skin; has blue or darkened lips, fingernails, and eyelids; is unable to sit still; does not respond when you call his/her name; has headaches; complains of no energy